
Muscle strains and tendinopathy are fairly common in athletes and the general population. However, it can be very tricky to treat or recover from them with no proper knowledge. Use the following as a rule of thumb to help in accelerating your recovery and getting you back to what you love pain-free.
- Education
- Discomfort is to be expected!!
- Adherence is key – chronic problems require chronic treatment
- Load management – complete rest is contraindicated because you will get:
- decrease muscle power/strength
- Tendon mechanical property degradation
- Kinetic chain movement deterioration
- Rest will immediately decrease pain but does nothing to correct the pathology present
- Avoid over stressing the muscle-tendon unit – don’t return to activity too quickly
- Exercise
- Pain control
- When clinicians say “use pain as your guide” this is what they mean:
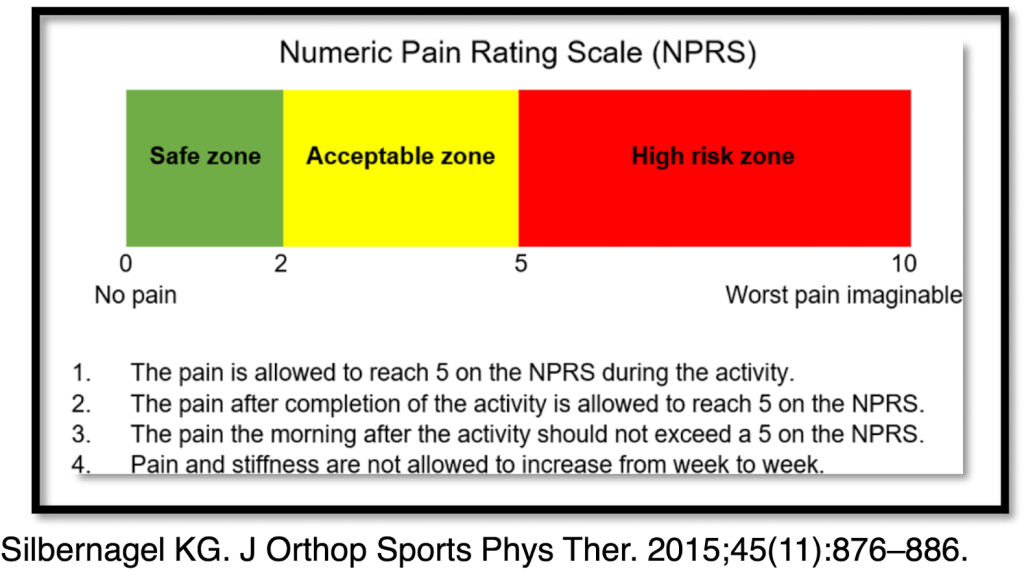
- on a scale from 0-10, 0 being no pain and 10 is the worst pain imaginable; your safe zone is 0-2, this is where you can do activity without feeling any pain.
- 2-5 is the acceptable zone.
- the pain is allowed to reach 5 on the NPRS during the activity
- The pain after completion of the activity is allowed to reach 5 on the NPRS
- The pain the morning after the activity should not exceed a 5 on the NPRS
- Pain and stiffness are not allowed to increase from week to week.
- 5 -10 is the high risk zone. This zone is typically not healthy for tissue healing.
- When clinicians say “use pain as your guide” this is what they mean:
Muscle strains
- A muscle strain is also known as a pulled muscle. It occurs when a muscle is stretched too far and part of it tears. It can be caused by overusing a muscle, using it incorrectly or an accident.
- Think of a muscle strain as a a frayed rope
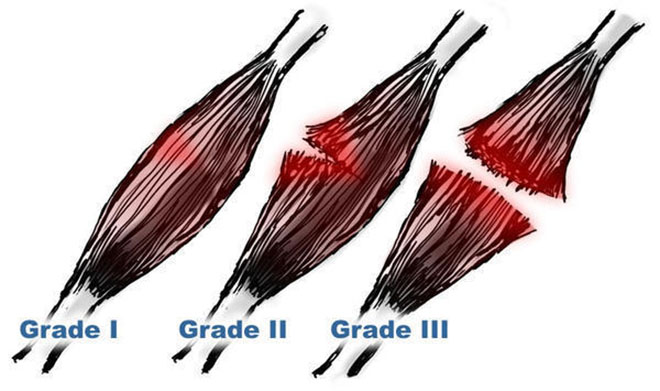
- Grade 1 – A few muscle fibers are frayed, similar to a rope with some frayed threads. There will be minor swelling and discomfort when the muscle contracts, but the muscle can still contract with normal strength
- Grade 2 – A significant amount of muscle fibers are frayed and some are torn, similar to a rope with a lot of frayed and torn threads. This is also known as a partial tear. There is a significant loss of strength and motion in the muscle, and there may be some swelling and bruising
- Grade 3 – the muscle is completely torn or ruptured, similar to a rope that is completely torn apart. This is also known as a complete tear. There is severe pain, swelling, and bruising, and the muscle cannot be used. This type of injury may require surgery
How to treat a Muscle strain
Interventions
- Stage 1 (Acute phase): The first 24-72 hrs you must pay the PRICE
- Protect
- Relative rest
- Ice
- Compression
- Elevation
- Stage 2 (3 days – 2 weeks): Reduction of acute symptoms
- Gentle range of motion (ROM) and sub-acute isometrics; modalities to reduce pain and swelling
- Start to introduce soft tissue mobilization to reduce restrictive scare formation
- Stage 3 (3-4 weeks): Pain-free isometrics
- Continue treatment as in stage 2; add strength, endurance and increase flexibility exercises
- Stage 4 (4-5 weeks): ROM 95% of normal, strength 75% of normal
- Begin sport-specific activities; emphasize coordination, agility and endurance
- Stage 5 (6-8 weeks): Strength 95% of normal
- Return to sport (RTS) with specific program to focus on proper warm-up, stretching and strengthening
Types of resistance Exercise: Why isometrics?
- During an isometric the muscle contracts to produce tension without change in overall muscle-tendon length
- no joint movement is produced
- Muscle portion contracts, tendon portion lengthens
- This is ideal for early stages of a strengthening program when muscle is weaker or if pain is a concern
- It is easier to teach and learn the concept of pain-free (or low pain) contractions with isometric exercises
- It may be tolerated better by patients with condition where shear forces may exacerbate the problem
- I.e. Arthritis, articular cartilage lesions
- Some recommend performance at multiple angles for better carry-over throughout the range (Brandy WD, Phys Ther, 1993)
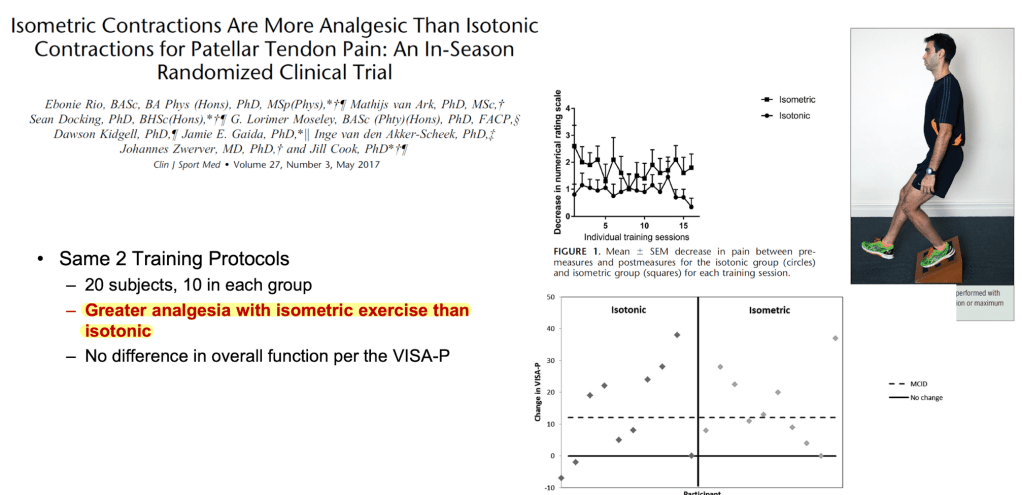
- Here is a comparison of isometric vs isotonic (muscle contraction with movement) in patients with patellar tendinopathy (Rio E et al, Br J Sports Med 2015)
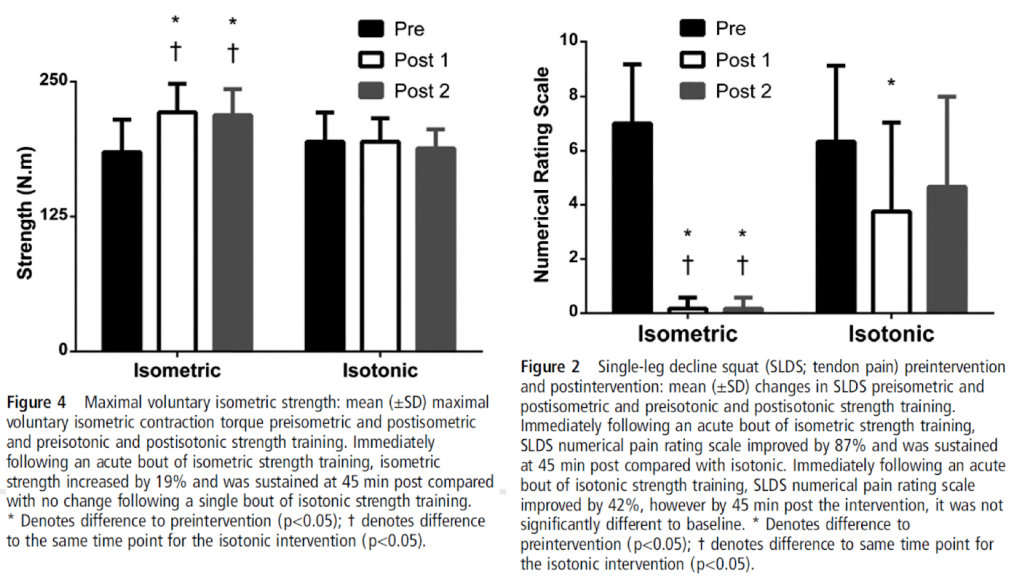
- To be fair, this is a very small sample size (n=6). Although, in the figure on the left it demonstrates time under tension was matched between isometrics and isotonics. However, the figure on the right demonstrates pain reduction and strength increase were greater with isometric exercise than with isotonic exercise
- immediate and 45 mins later
- In the same Randomized Clinical trail, the authors tested 20 subjects, and compared between isometrics and isotonics. Results showed that greater analgesia was associated with isometric exercises over isotonics
- Key take away: Isometrics are less painful with similar or greater strength increase.
Isometric exercise recommendations for pain-relief
- Mid-range is ideal to avoid compression at end range
- Hold for 30 – 45 seconds for 5 repetitions
- 2 min-rest between contractions to allow muscle (and brain) recovery
- Highly irritable tendons and low levels of function –> Body weight resistance
- Perform home exercise program
- Repeat more than once a day but consider 6 hours of rest between session
- Progress to larger external loads as appropriate
- Use pain to guide intensity – you don’t want to increase irritability
- Here are a few basic exercises you can perform at home with no equipment
- Quad sets 5 sets of 30-45 sec holds
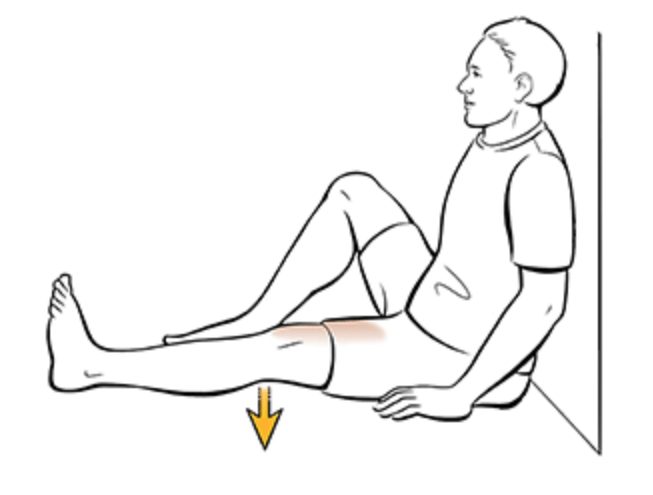
- Long arc quad hold at mid range 5 sets of 30-45 sec holds

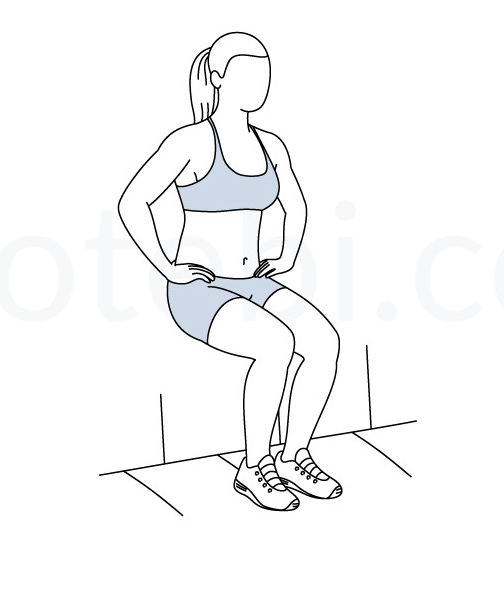
- Wall sits at 60 degrees of knee flexion 5 sets of 30-45 sec holds
What to do after Isometric exercise?
- Eccentric training
- initially proposed by Alfredson for Achilles tendinopahty
- Daily – 3 sets of 15 reps done SLOWLY
- Can be very irritating if not progressed properly
- initially proposed by Alfredson for Achilles tendinopahty
- Concetric training – Heavy Slow resistance
- Aim to induce collagen synthesis and can enhance the mechanical stiffness of the tendon
- Similar efficacy compared to eccentric exercises
- Achilles tendinopathy
- Patellar tendinopathy
- 4 sets of 6-8 reps on alternate days
- “isolated” movements when possible
- Isometric exercise may be needed as a warm up
- Eccentric: Concentric ration of 1:1 or greater
- Introduce endurance later on
Graduating to Speed and Sport

- Speed increases load on the tendon
- begin with body weight exercise before adding external load
- Check response to loading the next day with key test (one test repeated from baseline to finish i.e. double leg hops)
- Increased pain with the key test may indicate too much load
- Sport specific activities involve energy storage and release – make sure your body is ready
- Schedule Sample:
- Day 1 – Energy storage and sports specific activities
- Day 2 – cross training
- Day 3 – Heavy slow Resistance, Eccentric
- Repeat with rest as needed
Summary
- Muscle strains are pulled muscles, graded from 1 to 3, that occur from overloading, overstretching or an accident
- On the NPRS grades 2 to 5 are acceptable for muscle discomfort with rehabilitation and therapeutic exercise
- Injury recurrence is of particular concern. Structured programs with well defined clinical milestone allow a progressive, yet safe return to activity
- Isometrics > Eccentrics > Concentric exercises
- Late-stage revhabilaiton must include activities that achieve appropriate tissue loading thresholds that consider the speed of loading
- Overall quality of movement should be assessed and deviations that may predispose individuals to re-injury should be addressed


/GettyImages-569040885-56cdc4185f9b5879cc5bf429.jpg)


